

AI health tools are proliferating — ambient scribes, triage platforms, patient engagement solutions. But most assume infrastructure rural America lacks: reliable broadband, integrated EHRs, adequate staffing, and digital literacy.
A recent NEJM Perspective describes an 82-year-old woman living two hours from the nearest hospital. Her AI-enabled devices caught early fluid overload. The alert reached her daughter by text. But false alarms, spotty broadband, and fragmented care had eroded trust. She waited. By the next day, her mother was in respiratory distress.
The system was right. But the infrastructure to act wasn't there. And the message lacked context.
This week, I examine why AI tools fail resource-limited communities and how generative AI — designed correctly — could bridge the gap between clinical data and human understanding.
---
I spend a lot of time writing about AI tools that promise to improve clinical workflows — ambient scribes, triage platforms, patient engagement solutions. Most of these tools assume a baseline level of infrastructure: reliable broadband, integrated EHRs, adequate staffing, digitally literate patients.
That baseline doesn't exist in rural America.
A recent NEJM Perspective by Volandes, Davis, and Goldstein paints a sharp picture. They describe “Anna,” an 82-year-old living alone in a farmhouse two hours from the nearest hospital. Her AI-enabled scale and smartwatch flag weight gain and slowed gait (classic early signs of fluid overload). The alert reaches her daughter Maria by text. But false alarms (alarm fatigue!), unreliable broadband, and years of fragmented care have eroded Maria's trust. She waits until the next day, arriving to find her mother in significant respiratory distress from pulmonary edema.
The system was right but the message lacked context (how does the average patient or family member interpret a message about “weight gain” and “slow gait”?) And the infrastructure to act on it wasn't there.
This is the gap I want to focus on. We're building AI tools for healthcare environments that already have resources while leaving behind the communities that need them most.
Root Cause Analysis: 5 Whys
The 5 Whys process in root cause analysis involves repeatedly asking "Why?" five times to drill down into the root cause of a problem by exploring the cause-and-effect relationships underlying the issue.
The problem: AI-enabled health tools consistently fail rural and resource-limited populations despite being designed to improve care delivery.
Impact Analysis
Impact analysis is the assessment of the potential consequences and effects that changes in one part of a system may have on other parts of the system or the whole.
- Patient: Rural older adults managing multiple chronic conditions alone are the most vulnerable. Alerts sent to dead zones go unheard and interfaces with tiny fonts and unfamiliar symbols exclude patients with aging eyes and low digital literacy. The NEJM authors note that older adults in rural ZIP codes are 1.6 times more likely to lack in-home internet than their urban peers. Every missed alert chips away at trust and, trust, once lost in a rural community, is nearly impossible to rebuild.
- Clinician or Provider: Rural clinicians are already stretched thin. A nurse managing dozens of patients across hundreds of square miles could benefit enormously from AI triage but only if the tool actually works in that environment. When AI systems trained on urban ED documentation encounter a farmer who says "I'm feeling a bit poorly" (farmers are typically stoic!) they miss the urgency. Rural phrases like "I'll make do" confound NLP designed for direct urban communication styles.
- System: Rural hospitals are closing at an accelerating rate and EMS agencies struggle to respond. Meanwhile, the nursing shortage in rural areas is severe, and as the NEJM authors put it, the system can't hire its way out of it. If AI tools don't work in these environments, we're watching rural health care infrastructure collapse while sitting on technology that could help sustain it, but only if it's designed with these constraints in mind.
Solutions
The NEJM authors outline a table mapping four AI use cases in rural care against real-world constraints, risks of misalignment, and recommended alignment strategies. It's worth reading in full. Below are the four use cases.
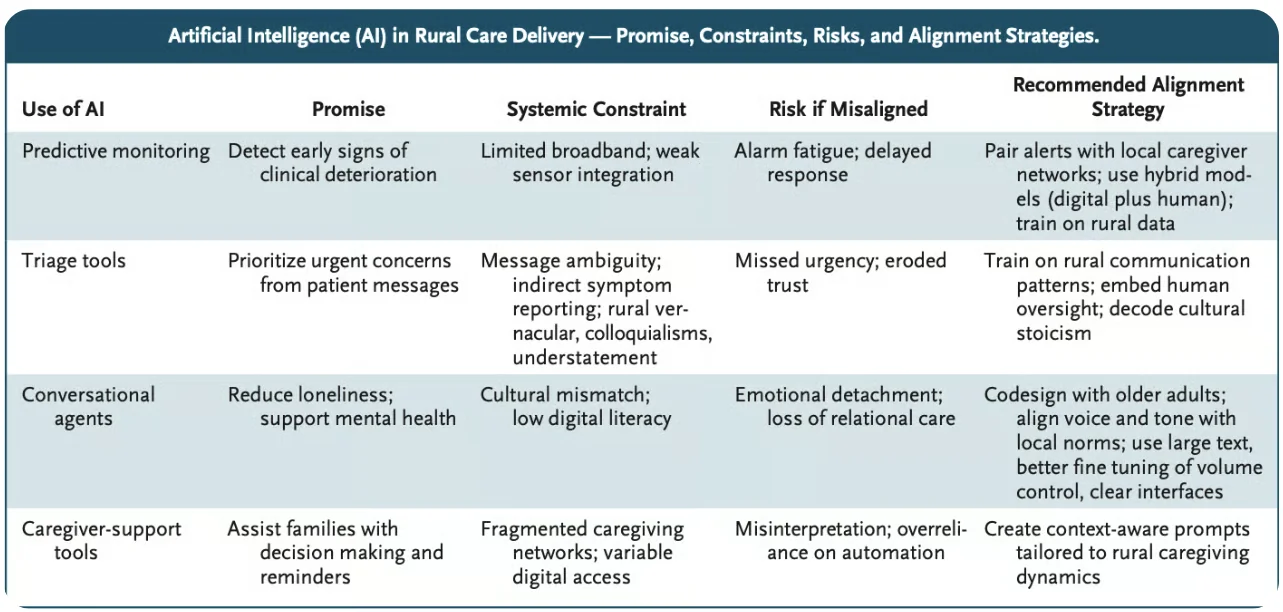
Source: nejm
But the solution I want to highlight is one that ties directly back to a topic I've covered before: using AI to make health information interpretable and actionable for patients and families.
In my article on AI-powered patient engagement, I wrote about the “dead zone” patients enter after clinical encounters. We discharge them with jargon-filled summaries, call them with results they don't understand, and tell them they have "community-acquired pneumonia" without explanation. The engagement challenge is closing gaps where patients fall through between hospital and home, diagnosis and understanding.
The NEJM authors describe the same problem, but in an environment where it's even worse. Rural patients face jargon and language barriers rooted in culture. AI systems trained on urban documentation miss the understatement baked into rural communication. And even when the AI parses correctly, the message may never arrive if broadband is spotty or the caregiver doesn't trust the technology.
Their proposed solution resonates: AI systems must offer actionable insights in plain language, accommodate local caregiving norms and infrastructure gaps, and support hybrid models that combine digital tools with human follow-up.
Consider their reimagined version of Anna's story. Broadband-equity funds reach her hillside. Her scale and smartwatch detect a 2-lb weight gain and slowing steps. Instead of raw data, the system sends a plain-English alert — "Possible fluid build-up" — to Maria's phone, with a single option to request a nurse callback. The alert also pings a community paramedic dashboard and the on-call nurse. Within minutes, a nurse explains the situation, confirms a paramedic is en route. The paramedic administers IV furosemide and schedules a same-day video check-in with Anna's cardiologist.
So, the same sensors and same data are used, but the outcomes are completely different, all because the system translated data into something a family member could understand and act on, and backed it up with a human.
This is where generative AI has real potential. Not in replacing the clinician or the caregiver, but in serving as the translator between raw clinical data and human understanding. A gen AI layer that converts "2-lb weight gain, decreased ambulatory speed, BNP trending up" into "Your mom may be retaining fluid, here's what to watch for and here's who to call" could be the difference between a managed episode and an ICU admission.
But it only works if we build it right. The authors argue—and I agree—that federal regulators should require developers to disclose the geographic distribution of their training data. Medicare should reimburse AI-enabled monitoring only when paired with documented human follow-up. And rural health systems need local AI governance boards—clinicians, patients, and community members who guide adoption based on cultural fit and social trust, not just performance metrics.
As I wrote in my patient engagement piece, transformative AI requires transforming the system, not just automating it. In rural America, that means we stop building tools that assume the infrastructure exists and start designing for the communities where it doesn't. The technology is there. The question is whether we'll deploy it in a way that strengthens the trust-based networks rural communities have always relied on or fracture them further.
Jared Dashevsky, MD, is an internal medicine physician and incoming pulmonary and critical care fellow at Mount Sinai, and the founder of Healthcare Huddle — a newsletter read by over 30,000 physicians and healthcare professionals. He writes at the intersection of clinical medicine, health policy, and health technology, translating complex industry dynamics into sharp, evidence-based commentary for busy clinicians. His work covers AI in practice, drug pricing, insurance dysfunction, and the business forces reshaping how medicine is delivered.
